

Q2 2026 at Lemons 🍋
Squeezed fresh for you: the latest from Lemons.

Hi everyone,
We want to share what’s happening in immersive health and inside our lab

Lemons Journal is where we explore how virtual reality, product design, and neuroscience are redefining healthcare.
The day the ground moved
On May 27th, two things happened before lunch.
In Rome, the Chamber of Deputies passed Italy’s first bill on digital therapeutics. 234 votes to 0. It now heads to the Senate for final approval.
For the first time, Italian law defines a digital therapy as a CE-marked medical-device software and opens the door to public reimbursement through the LEA.

That same morning, in Barcelona, we walked onto the main stage of the Health Revolution Conference and told hospitals across Spain what LEMO does.
Three weeks later, two of them were running it on real patients.
The direction is set. Q2 was about proving we can move inside it faster than anyone else.
The numbers

Live deployment as of today: 61 headsets. Zero churn since inception.
The top of the funnel has never been healthier. The gap is not demand. It is conversion speed.
The one red number
€38k closed against a €200k target. We are not going to dress that up.
It is a timing problem, not a demand problem. Italian public procurement runs slow. The €435k of proposals we sent this quarter convert next ones. We see the deals. We do not yet close them fast. That is the honest read.
The fix is already in motion. The sales team finished a structured training program and now runs on a real playbook: disciplined pipeline management, multichannel lead generation, a repeatable qualification-to-close process. Zero churn tells us the value is real once we are in. The job now is speed of entry. That is what Q3 carries.

What we said last quarter, and what actually moved
Customer Success became infrastructure. We stood up the department for real. Dedicated owner, goals, a playbook, not a side task. The blocker we flagged last time was nurse adoption, so that is exactly what we worked.
It moved. Doctors now prescribe LEMO and nurses run it as a daily routine, not a novelty. The proof is in the usage curve: minimum usage climbed from fewer than 30 sessions per two weeks to over 180.
Perceived value is no longer a hypothesis in these wards. It is observed behavior. On top of that, we ran our first fully remote onboarding. Training and onboarding are now digitized and tested end to end. Q3 is about scaling it.

Product delivered session depth. LEMO v0.5 is live: a substantial rebuild of the UX and patient journey, with tablet control fully adaptable across short and long procedures. Underneath it, LEMO Park, our pediatric line, is in production and nearly complete.
Clinical and Regulatory went to the top of the system. We sat down with AIFA and Agenas: a direct meeting with AIFA’s President and Agenas’s Director General, on digital therapies specifically. With MDR Class I in hand, the next steps on the roadmap are Class IIa and FDA clearance, the harder and higher-value certifications. HTA is now formally underway: the health economics that turn clinical outcomes into a procurement budget line.
Europe found its beachhead. Two active demos in Spain (Hospital Sant Pau, Vall d’Hebron), six qualified hospitals, a foothold in the Barcelona Health Hub. Spain is now our beachhead market. DACH stays on the roadmap. Q3 is about giving Spain structure.

The category nobody owns yet
Here is the whitespace, and it is worth understanding precisely.
The VR therapy that gets reimbursed today is home-use. One device carries a public reimbursement code, in the US, for chronic back pain, self-administered over 56 sessions on the patient’s couch. Useful. But it lives at home, after the hospital, alone.
The VR that lives inside the hospital, during the IV line, the CT, the wound care, the pediatric procedure, is sold as a distraction tool. Real clinical benefit, real hospitals, but off any reimbursement pathway. A cost line, not a covered therapy.
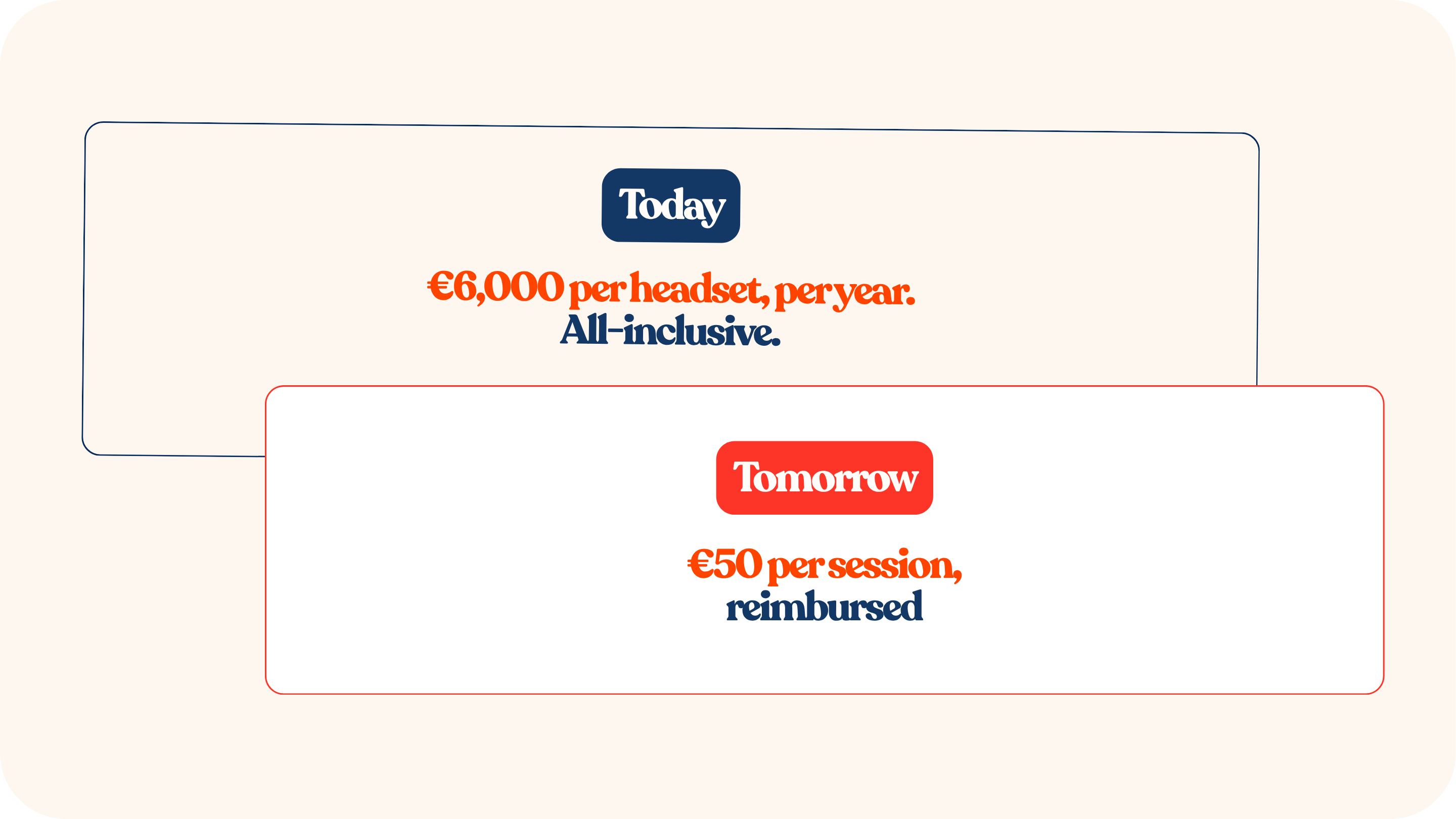
In-hospital plus reimbursed does not exist yet. That intersection is empty. That is the category we are building: the immersive therapy that lives where care actually happens, and that the system pays for as a therapy.
On May 27th, Italy passed the law that opens the door to exactly that. We are already inside 30 hospitals. The path to walking through that door has a name, and it is clinical evidence. Which is exactly where our next hires and our next capital go.
Fundraising
We are raising a €2M seed round. €650k is already committed.

That is roughly a third of the round closed before we opened it wide.
This capital goes into one thing: making LEMO the VR framework for the hospital. The clinical standard for immersive therapy, certified and defensible, and scaling it globally, the US included.
The round is moving. Allocation is filling.
Q3 priorities
This is a consolidation quarter. Three things, nothing else.
Density. Raise the average headsets per ward. Make immersive therapy a standard in care, not a pilot.
Health economics. Prove not just the clinical benefit but the financial one. Turn every anesthesiologist-hour and every avoided sedation into a budget-line argument.
Chief Science Officer. We have the profile in sight. This person owns clinical validation and the certification roadmap end to end. This is the hire that unlocks the category above.
How you can help
We move faster with you in the room. Right now we are looking for three specific things. Reply to this email and we take it from there.
Warm intros to seed-stage healthtech and digital-therapeutics VCs.
Clinical champions and KOLs in Spanish and EU hospitals.
Health-economics and HTA academic partners.
VR will not stay a pilot in the ward. It is becoming the clinical standard, and the window to own that category is now. We are already inside it.
Today the player. Tomorrow the standard.
From Lemons, with love 🍋